21 Years Since Son, Mike Died. Superpower: Accepting What Is
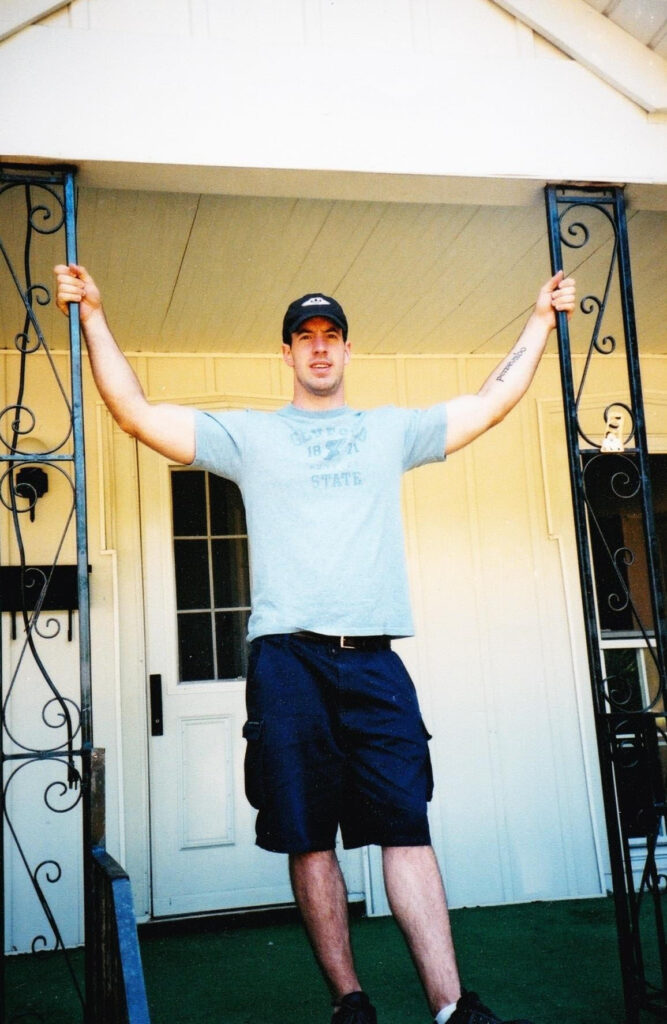

My son, Mike, died 21 years ago at age 26. Wasn't born with a tattoo…
Danny van LeeuwenNovember 18, 2023