
Podcast: Play in new window | Download (Duration: 35:02 — 28.1MB) | Embed
Subscribe: Apple Podcasts | Spotify | Email | RSS | More
PCORI’s Dr. Chue brings to light the complexities & challenges of conducting research, engaging stakeholders, and implementing findings in real-world settings.
About the Show
Welcome to Health Hats, learning on the journey toward best health. I am Danny van Leeuwen, a two-legged, old, cisgender, white man with privilege, living in a food oasis, who can afford many hats and knows a little about a lot of healthcare and a lot about very little. Most people wear hats one at a time, but I wear them all at once. I’m the Rosetta Stone of Healthcare. We will listen and learn about what it takes to adjust to life’s realities in the awesome circus of healthcare. Let’s make some sense of all this.
We respect Listeners, Watchers, and Readers. Show Notes at the end.
Watch on YouTube
Read Newsletter
The same content as the podcast but not a verbatim transcript. Could be a book chapter with images. download the printable transcript here
Contents
Introducing Dr. Amanda Chue 01:37. 2
Path to young adult mental health research 03:48. 3
Do comparators exist? 08:17. 4
Efficacy versus efficiency 11:29. 4
Dynamic tension – Parent engagement in research 12:52. 4
A word from our sponsor, Abridge 13:38. 5
Dissemination to those with lived experience 15:51. 5
Research results impacting clinical work or decisions 19:07. 6
Dynamic tension – CER and innovation 20:04. 6
Dissemination – sharing results 21:36. 6
Community implementation 22:51. 7
Stakeholder Advisory Panels 27:06. 7
Dynamic tensions in public engagement, dissemination, and implementation 30:09. 8
PCORI and public engagement 30:53. 8
Episode
Executive Summary
PCORI’s Dr. Chue brings to light the complexities and challenges involved in conducting research, engaging stakeholders, and implementing findings in real-world settings. It emphasizes the need for long-term partnerships with community organizations and the importance of addressing disparities in research representation. The dynamic tensions in various research and implementation aspects underscore the need for thoughtful and creative approaches to address complex healthcare issues effectively.
Proem

Image created in DALL.E
I treasure the dynamic tensions in life—for example, privacy and community, pathological optimism and catastrophizing, early adopter and skeptic. While not a researcher, I am personally and professionally neck-deep in research. Yet, despite my commitment to research, I’m a skeptic. Who’s it for? How can it aid decision-making? Who’s included in the research question, process, analysis, and dissemination? Where are the vested interests? Do we already have evidence yet have little will to implement, or does the bureaucracy or culture impede action? I will step in and highlight some dynamic tensions as the conversation flows.
What about research funding sources? What’s their perspective? What are the dynamic tensions? I asked my cronies at PCORI (Patient-Centered Outcomes Research Institute) to introduce me to a staff scientist specializing in comparative effectiveness research funding for emerging adults with mental illness. Dr. Amanda Chue kindly agreed to speak with us.

Image created on DALL.E
Introducing Dr. Amanda Chue
Dr. Amanda Chue received a BS in human development from Cornell University and a Ph.D. in clinical psychology from American University. She is a Program Officer for the Clinical Effectiveness and Decision Science program at the Patient-Centered Outcomes Research Institute (PCORI). In this role, she manages a portfolio of comparative clinical effectiveness research awards focused on meaningful outcomes for patients. Her portfolio includes several studies on clinical strategies for managing and reducing long-term opioid use for chronic pain and suicide prevention.
Podcast intro
Welcome to Health Hats, the Podcast. I’m Danny van Leeuwen, a two-legged cisgender old white man of privilege who knows a little bit about a lot of healthcare and a lot about very little. We will listen and learn about what it takes to adjust to life’s realities in the awesome circus of healthcare. Let’s make some sense of all of this.
Health is fragile
Health Hats: Amanda, thank you for joining me. I appreciate you taking the time. When did you first realize health was fragile?
Amanda Chue: My best friend’s mother was diagnosed with breast cancer in third grade. Her mother was in her early to mid-thirties. And at that point in my life, I’d had some grandparents who had passed from cancer. But it was not until my friend’s mom was diagnosed that it occurred to me that younger adults or even our parents could pass away from a terminal illness. I assumed at that point our parents would all get to reach older age. So, we watched my friend’s mom go through treatment, and very luckily, she beat cancer. It was an early lesson that health is fragile and good health at a younger age is not guaranteed.
Path to young adult mental health research
Health Hats: So, how did your career take a turn into young adult mental health research?
Amanda Chue: I’m a clinical psychologist and a program officer at the Patient-Centered Outcome Research Institute, PCORI. It was very fortunate that my research interests in mental health broadly aligned with the values at PCORI in identifying the key areas where evidence gaps exist and we can make a big difference in public health. We can all agree that youths have a mental health crisis. PCORI has taken charge of identifying areas where they can make a difference by supporting research to address this concern that’s been growing in recent years and then accelerated during the pandemic.
Evidence gaps
Health Hats: How does PCORI identify those evidence gaps?
Amanda Chue: We do this in different ways by looking through evidence synthesis – systematic reviews, seeing where the field has identified significant gaps. We conduct many stakeholder engagement gatherings. That means we try to figure out the key players in healthcare topics. Regarding mental health, we want to talk to various clinicians, psychiatrists, psychologists, other mental health providers, and different patient advocacy groups – for example, the National Institute of Mental Illness (NAMI) and patients. We make a lot of effort to reach out to patients and their caregivers. If we’re talking about youth, those you know, making those decisions about their healthcare, we want that information to be relevant to them and help inform those decisions that they ultimately make.
Health Hats: What gaps have been identified?
Amanda Chue: Within youth Mental Health we’ve had a few initiatives recently. PCORI sometimes will fund targeted funding announcements. These topics have been identified at PCORI through different mechanisms, including lots and lots of stakeholder engagement.
Some of the targeted areas within youth mental health we’ve recently funded are pediatric anxiety, adolescent suicide prevention, and brief interventions for adolescent alcohol use. We’ve seen an increase in anxiety disorders. We started to see the research results in about 2020, as sometimes research findings lag in real-time.
And even up to 2020, we’re seeing that adolescent anxiety has increased, and depression may be about 25%. And I can only imagine that those numbers will be even higher when we do post-pandemic evaluations. That pediatric anxiety announcement was pre-pandemic. So that was something that had been identified but certainly will be even more relevant today. Also, there’s the intersection of mental health and substance use. Everyone is concerned about suicidality among vulnerable populations, including adolescents.
Do comparators exist?
Health Hats: I’ve been involved with PCORI for 13 years, doing reviews, being on the board, and advisory panels. Comparative effectiveness research (CER) means that A is more likely than B to be effective with specific populations and settings. There are areas, especially when you get outside of medicine, where it’s hard to find comparators with research and evidence behind them. Let’s take the parent stakeholder as an example. I have had a family with severe depression. We asked to be involved in the treatment and recovery plan. The illness and the treatment were happening away from us, not with us. So, we didn’t know what to do in real life. There must be a research question, but I’m not sure there’s research to compare. Do you understand what I’m asking? How do you deal with cases where finding research comparators is hard?
Amanda Chue: It is undoubtedly challenging. I’ll remind you that our research tries to compare two efficacious treatments against each other or treatments in widespread use.
Health Hats: It’s called usual care, right?
Amanda Chue: Yes. So, I guess sometimes some kind of treatment is already being used, and maybe those involve parents or other caregivers. And perhaps it hasn’t had as much research attention, perhaps due to the research venue or the time the research happens, right? So, we ask what’s already happening in the healthcare system. How does that compare to this more manualized treatment that has demonstrated some efficacy? And then, is it worth it for the healthcare system to adopt to keep treatment as usual, or should there be a shift to adopt this other intervention that has gone through more stages of testing for efficacy?
Efficacy versus efficiency
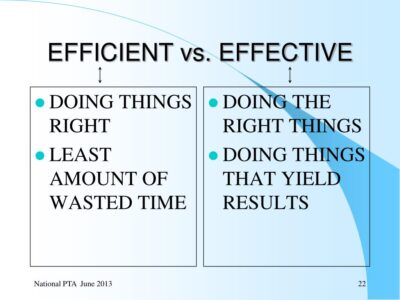
Slide by Mya Jonanthan, Local Unit Leaders How to Work Efficiently and Effectively
What is efficacy, and how does it differ from effectiveness and efficiency? Efficacy and effectiveness are similar. Doing the right thing yields results, while efficiency is doing something with the least waste of time and effort. See more in the show notes.
Dynamic tension – Parent engagement in research
Amanda Chue: So that’s one consideration. But regarding involving parents, we try to fund research where the treatments are realistic, right? So, things that families find useful as identified by engaging with the parents, caregivers, and youths to see what kinds of interventions they would be interested in. Sometimes we think about the CER question as a decisional dilemma, right? So, if you must choose between A or B, what evidence would you need to make that decision? We promote

image by Irina Shishkina on UnSplash
research around treatments that patients, caregivers, and parents would want to use or have access to.
Health Hats: Perhaps we have dynamic tension between privacy and parental engagement. Consider birth control, sexual identity, STDs, and mental illness. An article in Human Communication Research talks about Parent-Child Boundary Conflict. The paper describes four boundary conflict patterns: (a) combative, (b) guarded, (c) surrendered, and (d) trusting. Article in show notes. Worth the read.
A word from our sponsor, Abridge
Now a word about our sponsor, ABridge. Record your healthcare conversations with doctors and other clinicians with ABridge. Push the big pink button and record. Read the transcript or listen to clips when you get home. Check out the app at ABridge.com or download it from the Apple app store or Google Play store. Let me know how it went.
Call to action
I need help. I’ve expanded my podcast this year to include video, and costs have surged to $15,000 annually, while each episode takes 30 to 40 hours to produce. With growing content and shrinking bandwidth, I need support to keep creating without impacting our retirement funds.
As I look towards the next 5-10 years, I’m building a production team of emerging adults to carry this project forward. This succession planning requires resources. But here’s the deal: you can help.
Visit health-hats.com/support for ways to contribute. Best option? Patreon offers a monthly subscription with bonus content, Zoom meetings with me and fellow contributors, personal Bari Sax MP3s, coaching sessions, and more.
Occasional donations are welcome, and you can still subscribe for free to enjoy bonus episodes. You can also recommend us through email, social media, or postcard – postage on us! Visit health-hats.com/support. Your support is deeply appreciated. Thank you.
Dissemination to those with lived experience
Health Hats: That’s a great segue. In my seat on the PCORI board, I pay attention to dissemination and implementation. Research that doesn’t get out to people is ink on paper or bytes in the ether. We’ve spent all this money, so what? And it seems that it’s easier to think about disseminating to professional groups than to the public or people with lived experience. And it’s easier to disseminate than it is to implement. For me, changing habits is not easy. If a practice is a workflow or a life flow, habits are hard to change. I don’t know if we expect too much in how research can motivate change. So how does PCORI grapple with broad dissemination and implementation? Let’s take the example you said in one of the threads – that’s not the right word – One of the topics is adolescents trying to prevent adolescent suicidality and then think about dissemination and implementation using that example.
Amanda Chue: In part, it starts regarding the research idea and how PCORI evaluated research applications. There is an expectation that merit reviewers compare interventions already in use, already available in the healthcare systems. We start from a place where it’s not bringing in something brand new, right? Maybe it’s not used everywhere, but there should be available access. These are living interventions already used, so there’s some traction there. I think that helps. So, there is an expectation that these interventions are available already.
Research results impacting clinical work or decisions
Amanda Chue: In terms of dissemination and implementation, one of our criteria when applications go through merit review is will the findings from this study impact clinical work? Will it make clinical changes if there are significant findings from this study? So that’s something that’s already getting evaluated in the beginning. So even if we found that intervention A is better than B, would that make a difference to clinicians, healthcare providers, and patients who must decide? And sometimes there are cases where there are applications where it’s determined, even if we knew the answer to this question, it wouldn’t make much of a change. It’s so minor that that is a factor in whether it’s worthy or determined to be meritorious. So, we try to address some of these concerns in the beginning.
Dynamic tension – CER and innovation
Image by Tomas Sobek on UnSplash
Health Hats: Here’s another dynamic tension – between CER (comparative effectiveness research) and innovation. According to a 2019 New England Healthcare Institute white paper, fragmentation, localization, and misaligned incentives affect healthcare practices, organization, and delivery innovation. Let’s consider an example for emerging adults with mental illness. We’ve heard from Dorothy Cucinelli and Kelly Lane about the innovative COAST (Coordinated Opioid and Stimulant Treatment) program that provides 24/7/365 access to medication-assisted treatment and referrals to wraparound services for people with substance use and mental health concerns. How would a comparative study be designed? Each community, region, or state manages behavioral services differently (localization), wraparound services highlight fragmentation, and NY State aligned the incentives.
Dissemination – sharing results
Amanda Chue: In terms of dissemination and implementation, those are more of dissemination at this point in the application review process, but reviewers also look at that in the dissemination plan. Is it just to those standard scientific journals and conferences that it’s only going circulate to professionals, the other researchers, and that’s where our stakeholder advisory panels come in, right? We’re hoping that researchers can leverage their relationships with those stakeholders to help them think more broadly and creatively about how to reach the people we hope will get this research – other patients, clinicians, or advocacy groups. Do they already have relationships with those advocacy groups so that when the findings come out, they can distribute or disseminate them broadly so that more people can access them? We also evaluate our applicants on how creatively they can think about how to disseminate broadly.
Community implementation
Amanda Chue: Yeah. Implementation’s a little harder, I think, or a lot harder. Again, we hope that the interventions we’re testing, as I said, are in the healthcare system. We expect the evidence generated after the study to be impactful and might develop or influence changes in healthcare policies. But how that link happens that’s a little trickier.
Health Hats: I interviewed these folks from a community health agency with drop-in centers for at-risk youth. I asked them what questions they had that they thought that research could help them. And they, now I’m putting words in their mouth. It’s a combination of what they said and what I think. So, I’m transparent: they said we know what works. The challenge is doing it. The challenge isn’t so much answering questions. They know that the most critical thing is that people feel safe and belong. They don’t need research to tell them what’s important, but that doesn’t make it any easier. That there are forces in play that make things hard to implement. One of the things I like about PCORI, which drew me to PCORI, was being at the forefront of including people with lived experience at every step of the research process. And it’s risky. It’s scary, and when it works, it’s gold. So, suppose the populations we care about in this are emerging adults, children, incarcerated people, people without permanent housing, or people with cognitive challenges. In that case, these are all like there are challenges to including people every step of the way. And you need to be bold and take chances when you do that. How has that impacted your work? In terms of working with people who are applying or are successful in their application for research to include those, I’m a two-legged, cisgender old white man, a privilege. I get invited to all sorts of tables. That’s all I know. I’m not representative of much, just that slice. How do you guys help that evolve?
Stakeholder Advisory Panels
Amanda Chue: Yeah. That is an excellent question regarding how we can be inclusive within our stakeholder advisory panel. Not just inclusive of the different stakeholder groups, but within patients, how do we make the patient representation on any stakeholder advisory board representative of the sample we’re hoping to address in this research? That’s hard. That’s a tricky question. And I think I was even thinking about our topic with youth, right? I think it’s much easier to try to engage adolescents, but if it’s a study on younger kids, that is trickier.
Health Hats: It’s easier to go with your parents. But this is good because parents are essential stakeholders. But this is early on. Still, when I like to talk with people with lived experience, I don’t say anything I’m saying is generalizable. Still, there’s more hopefulness in people living it and working with people directly living it than with the stakeholders, who are insurers, provider organizations, or hospital systems. Having those stakeholders around the table might open more possibilities. I don’t know. Engagement can be a fraught area.
Amanda Chue: It is challenging. I know there’s an emerging science of engagement efforts even within PCORI, and we’re like what you’re saying we know this works. How do we provide evidence to show the mechanisms that make it work? Then it’s replicable for others, right? What are the ingredients that make stakeholder engagement work? And I think there are still needs, maybe in the early days around that. I hope we can start to identify some pieces around how to engage more vulnerable populations, perhaps in the research conducted for them. We can hear their voices. And these are maybe harder to reach or engage for various reasons.
Dynamic tensions in public engagement, dissemination, and implementation

Image by Muhammad Nasir on UnSplash
Funders award a researcher’s project for a limited time-a year, two or five. The award covers direct and indirect costs – research expenses, cost of the infrastructure, and institution. Implementation often takes more than two to five years – tension. Researchers don’t usually have dissemination and implementation skills. They’re researchers. It’s like expecting teachers to raise our kids. They’re teachers, not parents.
Community partnership-building skills also vary with the researcher – another tension. Those that build relationships and networks as part of their routine or have mentors and support systems to guide them have a leg up on those who don’t.
Some research-public engagement partnerships lend themselves to automatic implementation. But implementation can occur locally, but not beyond (region, state, country, cultures). Indeed, a dynamic tension.
Can you come up with more?
PCORI and public engagement0
Health Hats: There’s a strong contingent of people who would like to be part of the research, and then they hear about PCORI. The few who have listened to PCORI may think we should get involved. And then it’s just so daunting, the idea of applying. And what I do is encourage people to partner with researchers and establish long-term relationships. And then, on the other hand, it’s, when I know research groups, I try to hook them up with. Community people that I know so that they can begin to develop or continue to develop or expand those relationships. So how do, like now, you think about this young adult mental illness, whether it’s a suicidality prevention or a reduction? How does PCORI approach that business of partners, like long-term partnerships with community organizations?
Amanda Chue: Are you familiar with our different engagement awards? There? There are a couple of different levels. We have the Eugene Washington PCORI Engagement Award program.
Health Hats: There was a Pipeline to Proposals a few years ago. That was exciting. It was a staged thing, wasn’t it? Organizations could prepare to partner. Then some grants were building a partnership and then sustaining a partnership. And I liked that this graduated iterative was maturing together and supporting that effort.
Amanda Chue: Our current engagement awards include awards for stakeholder convening support. So that might be an advocacy group applying for this award to get funding to gather all the relevant stakeholders so that they can, I guess, create an effort where they’re maybe really thinking about the critical evidence gaps towards whatever healthcare issue they focus on. So that’s a starting point to help generate some of those. Identifying those key evidence gaps will hopefully lead to research proposals that aim to address them. Then there are also capacity-building cards, th. These projects support organizations with strong ties to patients, caregivers, clinicians, and other stakeholders connected to a research focus area. And this award is meant to be a bridge to equip the stakeholders better to engage as partners in research. So that might be that intermediary stuff.
Health Hats: I like that simultaneous focus on infrastructure. That’s what I would put that it’s different than the infrastructure of an academic medical center, which certainly has plenty of money. But the building of the integrated infrastructure.
Policy making
The last thing that maybe, or the second or the final, okay. Occasionally, I will talk to a congressperson’s office. I can’t say that I’ve ever spoken to a Congress person directly. But the people in their office and related to PCORI, one thing they say is that they need research to inform their policy-making. What you were saying before, which I’ve already forgotten except for the suicidality thread, is so, what do you think are in this young adult and mental health portfolio? What is there that will help policymakers?
Amanda Chue: One area I think could help to address youth mental health; we can all agree that there’s been a shortage of mental health services and providers. One means to address this concern to some extent is telehealth, the expansion of telehealth which could increase access. And as you might know, during COVID, some of the restrictions around telehealth were Loosened to provide this need that suddenly emerged.
But we’re still trying to, I think, synthesize the evidence to show that telehealth is just as good as in-person care. Okay. And so I think that’s one area where we could generate more synthesis around or synthesize that research to demonstrate the efficacy or effectiveness of telehealth. And I think that’s an area, Okay. That could have policy implications, right? Will insurance coverage for telehealth continue once the public health emergency phase ends as scheduled in January of this year?
Great. And so that will have implications on what kind of telehealth services continue to be covered, I guess federally, which has trickle-down effects on all the private insurers.
Wow. Thank you. This has been lovely.
Amanda Chue: Yeah. Thank you. It’s really. It’s an honor to also speak with a board member as a PCORI staff member. We don’t have a lot of interaction and not in this kind of venue by any means. It’s been a pleasure getting to spend some time with you.
Health Hats: Thank you.
Reflection
Image created in DALL.E
As I began producing this episode with Dr. Chue, I worried readers, listeners, and watchers might find this topic dry and remote. I found value in including the research funder’s perspective to complete a picture of emerging adults with mental illness. Dr. Chue and my conversation led me to highlight the dynamic tensions in research. Science has complexities as does life. We identified the tensions between parental engagement and privacy; CER and innovation; duration of studies and implementation time, cost, and expertise; community partnership building skill and research; and local implementation and generalization to other communities.
I also found the concept of implementation more challenging and complex now than when Dr. Chue and I spoke. I should have known better. I agitate for implementation in my Board seat, yet I well know that implementation means change of habits, culture, and incentives. For professionals, clinics, organizations, and health systems, that means changing workflow and power dynamics, and for the public changing life flow and sometimes community. So daunting. Can you think of anything more so? I need to reflect some more. Thank you, Dr. Chue.

Image by Benjamin Wedemeyer on UnSplash
I have one more episode recorded with Sherry Wang, a health economist. I’m hoping to add an episode about cultural variation and then wrap up with a summary episode. That will be 16 episodes in the series. Yikes.
Podcast Outro
I host, write, edit, engineer, and produce Health Hats, the Podcast. Kayla Nelson provides website and social media consultation and manages dissemination. Joey van Leeuwen supplies musical support, especially for the podcast intro and outro. I play bari sax on some episodes alone or with the Lechuga Fresca Latin Band. I’m grateful to you, who have the most critical roles as listeners, readers, and watchers. See the show notes, previous podcasts, and other resources through my website, www.health-hats.com, and YouTube channel. Please subscribe and contribute. If you like it, share it. See you around the block.
Episode Notes
Please comment and ask questions
- at the comment section at the bottom of the show notes
- on LinkedIn
- via email
- YouTube channel
- DM on Instagram, Twitter, Mastadon to @healthhats
Production Team
Web and Social Media Coach, Dissemination Kayla Nelson @lifeoflesion
Leon van Leeuwen edits the article-grade transcript.
Music on intro and outro by permission from Joey van Leeuwen, Drummer, Composer, and Arranger, including Moe’s Blues for Proem and Reflection and Bill Evan’s Time Remembered for on-mic clips
Other Credits
Images
Vulture Couple by Rich Rieger, used with permission
Woman and Clown by Diana Feil on Unsplash
A tall rock in the ocean image by Irina Shishkina on UnSplash
Close-up of 2 zippers image by Tomas Sobek on UnSplash
Monkey on camera image by Muhammad Nasir on UnSplash
Painter sitting on a schoolbus image by Benjamin Wedemeyer on UnSplash
A person with colorful particles coming out of their body image created in DALL.E
Disclaimer
The views and opinions presented in this podcast and publication are solely my responsibility and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute® (PCORI®), its Board of Governors, or Methodology Committee. Danny van Leeuwen (Health Hats)
Sponsored by Abridge
Inspired by and grateful to Mike Herndon, Bill Lawrence, Joanna Siegel, Marv Feldman, Robert Motley, Adam Thompson
Links
Amanda Chue PCORI
PCORI Clinical Effectiveness and Decision Science
Eugene Washington PCORI Engagement Award
What is efficacy, and how does it differ from effectiveness and efficiency?
Dynamic tension between privacy and parental engagement
Human Communication Research talks about Parent-Child Boundary Conflict.
According to a 2019 New England Healthcare Institute white paper, fragmentation, localization, and misaligned incentives affect healthcare practices, organization, and delivery innovation.
Related podcasts
Series: Pediatric Transition to Adult Care
Creative Commons Licensing
The material found on this website created by me is Open Source and licensed under Creative Commons Attribution. Anyone may use the material (written, audio, or video) freely at no charge. Please cite the source as: ‘From Danny van Leeuwen, Health Hats. (including the link to my website). I welcome edits and improvements. Please let me know. danny@health-hats.com. The material on this site created by others is theirs, and use follows their guidelines.